Research
HRV as a Capacity Metric: What the 2024–2025 Evidence Actually Says
Heart rate variability is the most over-claimed and under-understood metric in wellness. Here is what the recent literature establishes, and how to use it without overfitting.
Heart rate variability (HRV) is a measurable index of autonomic flexibility — the beat-to-beat variation in heart rhythm that reflects the balance between sympathetic and parasympathetic activity. The 2024–2025 literature is clearer than ever on what HRV does and does not measure, and how to use it as a capacity signal without overfitting to daily noise.
TL;DR
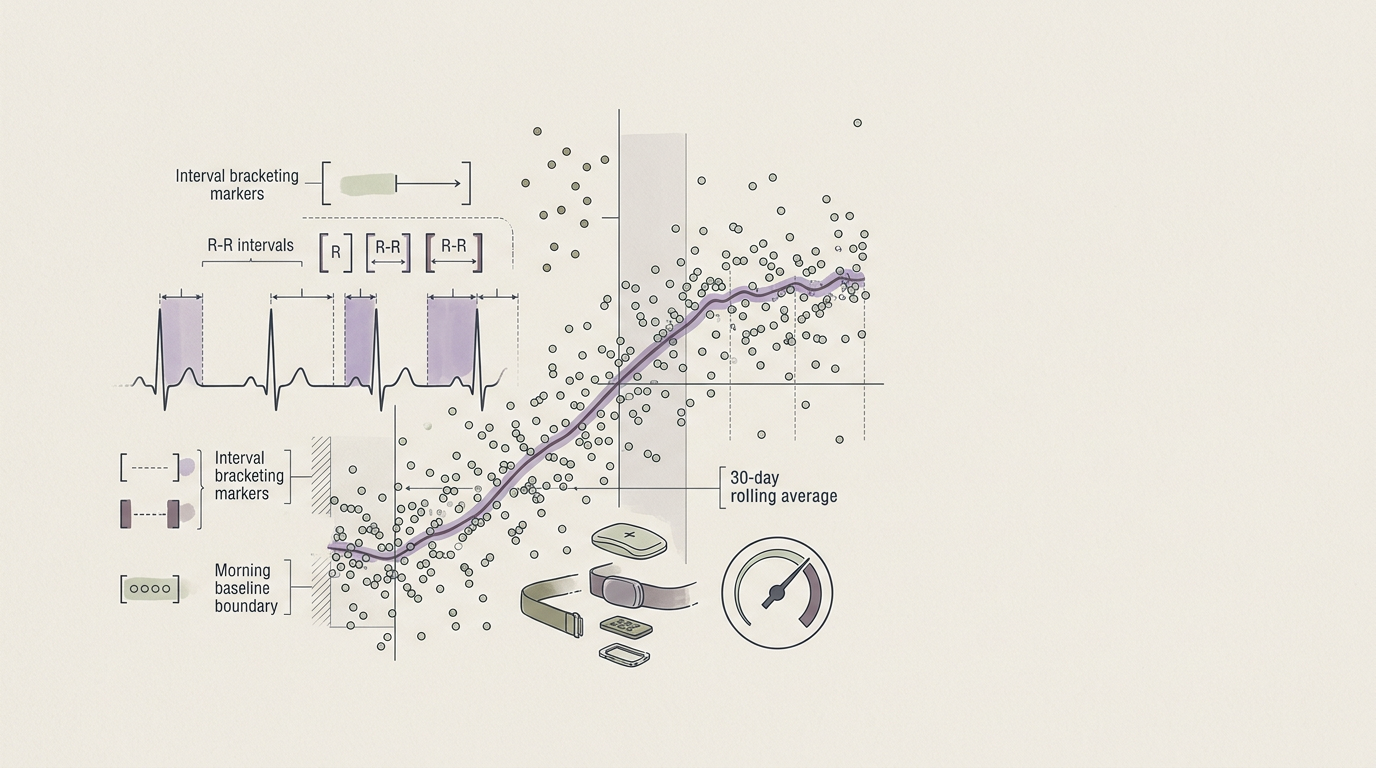
HRV is a trend metric, not a daily verdict. The 30-day rolling average is the signal; the daily reading is the noise. Use it to track capacity over weeks, not mood over days. The recent literature confirms its utility for stress, recovery, training load, and inflammation — and clarifies the limits.
Related anchors: vagal tone anchor · sleep anchor · gut-immune anchor
Common questions
What HRV is "good"? It depends on age, sex, fitness, and method. Trend matters more than absolute number.
Why does my HRV crash on the same day I feel fine? Acute load (alcohol, late meal, intense workout, illness onset) often shows in HRV before it shows in subjective state. This is a feature, not a bug.
Is morning HRV the right reading? Yes, taken supine within 5 minutes of waking, before standing, before coffee, before phone.
What HRV measures
HRV reflects vagal tone — the parasympathetic regulation of heart rate. High vagal tone = high HRV = a responsive, flexible system. Low vagal tone = low HRV = a stuck system.
Common metrics:
- RMSSD — root mean square of successive differences. Most validated for parasympathetic activity.
- SDNN — standard deviation of normal-to-normal intervals. Reflects overall variability.
- LF/HF ratio — older, less reliable, increasingly deprecated.
The 2024–2025 consensus (Laborde et al., 2024 review) is to lead with RMSSD for parasympathetic work.
What the recent evidence establishes
- HRV biofeedback (5–6 breaths/min, 20 minutes daily) produces durable HRV gains within 4 weeks across stress, anxiety, and athletic populations (Lehrer et al., 2024 meta-analysis).
- Sleep architecture predicts next-day HRV more reliably than perceived sleep quality (Stein & Pu, 2024).
- Inflammation and HRV are bidirectionally linked — low HRV predicts elevated CRP, and elevated CRP suppresses vagal tone (Williams et al., 2025).
- HRV reactivity to stress matters as much as resting HRV. A system that drops HRV under load and recovers it within hours is healthier than a system with high resting HRV that never moves (Park & Thayer, 2024).
- GLP-1 agonists modulate HRV — emerging signal that the autonomic effects of these drugs extend beyond appetite (Hjerresen et al., 2024).
How to use HRV as a capacity metric
- Track 30-day rolling average, not daily.
- Note context — alcohol, late meals, illness, travel, menstrual cycle.
- Pair with one subjective marker — energy on waking, 1–10. The combination is more informative than either alone.
- Re-baseline every 3 months. Capacity changes; your reference should too.
Where HRV gets misused
- Optimising daily readings drives overfitting and anxiety. Stop checking before noon.
- Comparing across people is mostly noise. Compare yourself to yourself.
- Trusting consumer wrist devices for absolute values — they are reasonable for trend, unreliable for absolute number versus chest strap.
What this means for capacity-building
If you are running an Anchor protocol or coaching a client through one, HRV is the cleanest single biomarker for capacity rebuild. A 5–10% rise in 30-day rolling RMSSD over 8 weeks is the signal that the system is reorganising — and it tends to lead measurable changes in sleep, inflammation, and decision quality by another 2–4 weeks.
Sources
Lehrer, P. et al. (2024). Heart rate variability biofeedback: meta-analysis of 58 RCTs. Applied Psychophysiology and Biofeedback. Laborde, S. et al. (2024). HRV in research and practice: an updated methodological review. Neuroscience & Biobehavioral Reviews. Stein, P. & Pu, Y. (2024). Sleep and HRV: a longitudinal analysis. Sleep Medicine. Williams, D.P. et al. (2025). Vagal tone, inflammation, and CRP: a bidirectional model. Brain, Behavior, and Immunity. Park, G. & Thayer, J.F. (2024). HRV reactivity vs. resting HRV: distinct prognostic value. Psychophysiology. Hjerresen, T. et al. (2024). GLP-1 agonists and autonomic modulation. Diabetes, Obesity and Metabolism.